
The critical gap - why musculoskeletal health is the forgotten ‘critical risk’.
There has been a lot of discussion lately about ‘critical risks’—those hazards that lead to death, or serious, notifiable injury. We all agree that New Zealand’s workplace fatality record is a serious issue that needs urgent attention, but by focusing only on critical risks, in the process we seem to be minimising the impact of work-related health issues such as musculoskeletal disorders (MSDs).
The real cost of sprains and strains
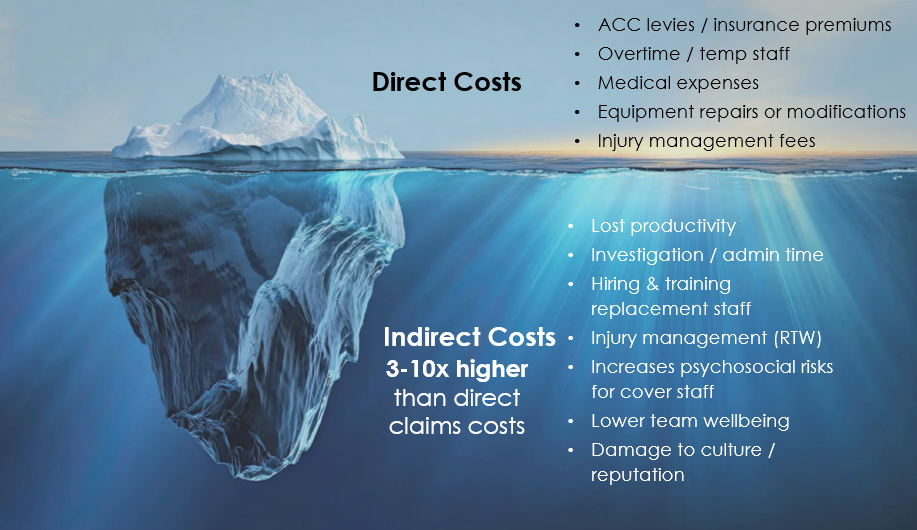
The visible cost of an injury is just the tip of the iceberg; indirect costs are often 3-10 times higher⁴.
Despite making up around 30% of all workplace harm in Aotearoa¹, musculoskeletal disorders are not typically classed as critical risks. But neither are they just minor issues. They are the primary driver of ACC claims and lost productivity. The Business Leaders Health and Safety Forum estimated that work-related harm costs our economy around $5.4 billion annually². Given the high rates of musculoskeletal harm, it is logical to assume a large proportion of that estimate could be attributed to musculoskeletal disorders.
But it’s not just about the money. It’s about the human cost. These injuries affect every part of a person's life, wellbeing, and community. The impacts ripple out, affecting business profitability and placing more pressure on our already stretched healthcare system.
Despite the scale of the issue, work-related musculoskeletal disorders (WRMSDs) are usually considered non-critical. This is a problem. These injuries usually develop slowly through long-term exposure to factors such as biomechanical or physical, work organisation, psychosocial, environmental, or individual risk factors³. Even when an injury happens during a one-off event, like a slip or trip, it usually ends up in the ‘non-critical’ pile.
It is easy to see why businesses prioritise their budget for things that can kill people. That is obviously vital. But it should not come at the expense of addressing things that cause chronic discomfort, pain, or injury; nor should it diminish a business’s basic duty of care under the Health and Safety at Work Act. Musculoskeletal issues are often dismissed as ‘just part of the job’. We risk creating a culture that ignores these slow-burn injuries until a worker cannot walk easily, pick up their kids, or is forced to leave the workforce entirely. This approach is short-sighted. As a nation, we need to stop relying on ineffective manual handling training and focus on the root causes, rather than just patching people up and sending them back to the same work that caused the harm.
Beyond the lifting poster – the compliance trap

Generic manual handling training is one of the most common approaches to preventing musculoskeletal harm or responding to workplace injuries. Yet, the science repeatedly proves it is not effective when used as a primary control on its own. Systematic reviews of evidence show that simply teaching people ‘correct’ lifting techniques has almost zero impact on long-term injury rates⁵.
Humans are not robots. We get tired, we take shortcuts when we are busy, and the work environment itself often forces people to adopt awkward postures, making the ‘correct’ technique impossible. This becomes even more precarious when you layer on psychosocial risks; pressure from high job demands or rushing doesn't just lead to mental stress—it causes physical muscle tension and reduces the cognitive 'buffer' needed to perform tasks safely. In a poorly designed system, a moment of fatigue or a rush to meet a deadline doesn't just lead to a strain; it can have fatal consequences. This is why manual handling training alone fails; it relies on a person to do the right thing every single time, regardless of the pressure they are under. It simply does not reduce exposure to the actual risk factors or prevent WRMSDs⁵.
Many businesses believe they must provide manual handling training as a specific legal requirement, but this is not actually the case in New Zealand or Australia⁵. That is not to say a business does not have a duty of care to manage the risks associated with WRMSDs; it absolutely does. The trap is thinking the generic training covers that duty.
Another issue with relying on manual handling training is that the individual is often blamed when they get injured. In reality, most injuries occur from repeated exposure to a range of risk factors. This does not mean we should provide no training at all. There is still a place for teaching the basics of how to move and handle things safely as one of many controls. Think of it as a foundational knowledge that supports a worker, but it does not replace a well-designed work system.
Effective training should focus on worker engagement throughout the entire risk management cycle—from identifying sources of risk to effectively controlling them. It should teach people how to perform tasks safely by understanding work procedures and how to use the specific tools and equipment provided. Crucially, it should also cover how to report niggles early and how to flag maintenance issues before they lead to an injury in order to support early intervention⁵. This shift in focus, from perfect lifting to early reporting and better design, is where we start to see real change.
‘Have a hmmm’ – the impact of injury on others
Most people in New Zealand have seen the ACC ‘Have a hmmm’ adverts. They are clever and catchy, and work well to get people thinking about how an injury impacts those around them⁶.
While 'Have a hmmm' might work for a weekend warrior on a ladder, it’s not the best strategy for a business managing musculoskeletal risks. If we want to support people’s physical and mental wellbeing at work, we need to move away from placing the burden on the individual. Instead, we must look at good work design as part of a risk management approach. While workers have health and safety responsibilities, they also need to receive suitable training and education, combined with systems that are well-designed to support them to work safely.
The need for a joined-up system

There is a real opportunity in New Zealand for our agencies to work better together. Currently, we have WorkSafe as the regulator and ACC as the insurer. While both play vital roles, there is often a gap between practical guidance for businesses, the funding available for injury prevention, and the support provided when people get injured⁷.
To truly address musculoskeletal health, we need a joined-up approach. Imagine the impact if the regulator, the insurer, and businesses all worked better together and focused on the same goal. By shifting the conversation from ‘fixing the worker’ to improving the work, we create a system that is consistent and supportive. When we work together to understand the entire work system, identify the root causes of risk, and introduce evidence-based interventions, we build a more resilient and productive Aotearoa.
Moving forward - What businesses can do
If the current national strategy relies on individuals to ‘have a hmmm’, and the Regulator has not provided a clear strategic lead, where does that leave you? If you are ready to move from being reactive to proactive—shifting away from relying on generic manual handling training as your only control—how do you actually manage musculoskeletal risks effectively?

Do not wait for a label.
Just because a hazard might not be legally classed as a ‘critical risk’ doesn't mean it isn't critical to your operation. The cost of turnover, ACC levies or AEP costs, and lost productivity from musculoskeletal harm will always hurt your bottom line.
Focus on design, not behaviour.
Stop telling people to ‘be careful’ and start asking ‘how can we make this task easier?’ Listen to your frontline workers; they are the experts in where the niggles are.

Integrate physical and mental health.
Recognise that a stressful workplace is a physically dangerous workplace. Using a holistic approach, like the Contributing factors for discomfort, pain, and injury/WRMSDs³ and the Te Whare Tapa Whā model⁸, allows you to address factors such as workload, work demands, support, and communication as part of your injury prevention strategy.
Aim for the ‘Goldilocks zone’.
Emerging research, such as the CoWork model⁹, suggests we should design work that provides ‘just the right amount’ of physical activity—enough to keep the body resilient without causing strain.

Get professional help.
Ergonomics isn't just about desks and chairs—it is about the whole system. A professional can help you proactively manage musculoskeletal risks by looking at your data, understanding the root causes, assessing the high-risk tasks, and find practical, evidence-based solutions that actually work.
The bottom line
While the national conversation continues to focus on a narrow set of 'critical risks', we cannot afford to ignore the large proportion of our workforce currently struggling with musculoskeletal harm.
Let’s stop being the ambulance at the bottom of the cliff, patching people up only to send them back into the same poorly designed jobs. It is time to treat musculoskeletal health with the urgency it deserves—not because of a legal label, or meeting minimum compliance standards, but because protecting the physical longevity of our people is simply good business.
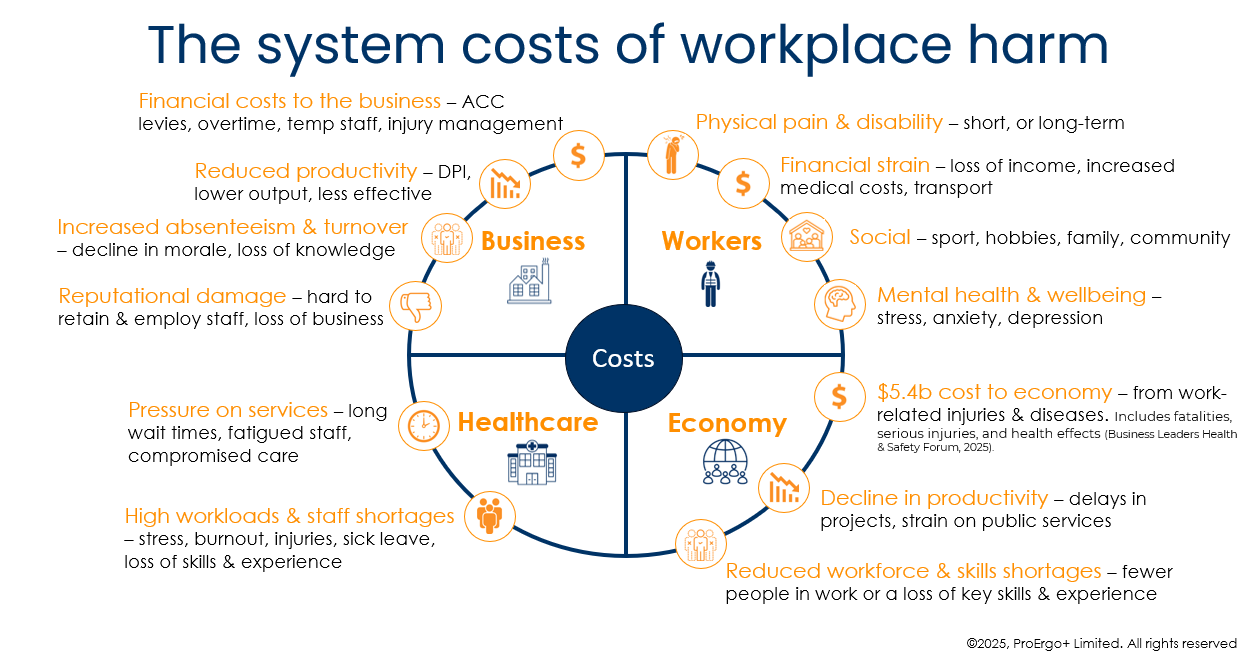
Musculoskeletal harm doesn’t just sit on a balance sheet; it creates a cycle of cost across the entire New Zealand ecosystem.
References
WorkSafe New Zealand. (2019). Burden of estimated harm from work-related ill-health.
Business Leaders Health and Safety Forum. (2025). State of a thriving nation.
WorkSafe New Zealand. Quick Guide: Work-related musculoskeletal disorders and risk factors.
Occupational Safety and Health Administration (OSHA). $afety pays individual injury estimator. Based on MCCI average claim costs data (2015-2017) and Business Roundtable indirect cost research.
Heads of Workplace Safety Authorities Australia & New Zealand. Heads of Workplace Safety Authorities position on ‘How to lift’ training.
Accident Compensation Corporation. (2026). About ‘Have a hmmm’.
WorkSafe New Zealand. (2025). Musculoskeletal health risk management: WorkSafe 2021–2024.
Ministry of Health/Manatū Hauora. (2023). Te Whare Tapa Whā model of Māori Health.
Holtermann A, Sørensen OH, Jacobsen SS, Lindberg L, Andersen LL. Beyond risk reduction of work-related musculoskeletal disorders: The CoWork musculoskeletal health model. Scand J Work Environ Health. 2025 Dec 2:4262. doi: 10.5271/sjweh.4262.